If you have feedback, let us know.
IPCCC ICD-11 Congenital Heart Atlas
- Structural developmental anomaly of heart or great vessels
- Congenital anomaly of position or spatial relationships of thoraco-abdominal organs
- Anomalous position-orientation of heart
- ■ Usual atrial arrangement
- Abnormal atrial arrangement
- Abnormal ventricular relationships
- Abnormal relationship of great arterial roots
- ■ Aortic root directly anterior to pulmonary root
- ■ Aortic root anterior and rightward to pulmonary root
- ■ Aortic root anterior and leftward to pulmonary root
- ■ Aortic root side by side and directly rightward to pulmonary root
- ■ Aortic root side by side and directly leftward to pulmonary root
- ■ Aortic root directly posterior to pulmonary root
- ■ Aortic root posterior and rightward to pulmonary root
- ■ Aortic root posterior and leftward to pulmonary root
- Abnormal intrapericardial course of great arteries
- Visceral heterotaxy
- ■ Total mirror imagery
- Congenital anomaly of an atrioventricular or ventriculo-arterial connection
- ■ Concordant atrioventricular connections
- Discordant atrioventricular connections
- Transposition of the great arteries
- ■ Transposition of the great arteries with concordant atrioventricular connections and intact ventricular septum
- ■ Transposition of the great arteries with concordant atrioventricular connections and ventricular septal defect
- ■ Transposition of the great arteries with concordant atrioventricular connections and ventricular septal defect and left ventricular outflow tract obstruction
- Concordant ventriculo-arterial connections
- Double outlet right ventricle
- Double outlet right ventricle with subaortic or doubly committed ventricular septal defect and pulmonary stenosis, Fallot type
- ■ Double outlet right ventricle with subpulmonary ventricular septal defect, transposition type
- ■ Double outlet right ventricle with non-committed ventricular septal defect
- Double outlet right ventricle with subaortic or doubly committed ventricular septal defect without pulmonary stenosis, ventricular septal defect type
- ■ Double outlet right ventricle with intact ventricular septum
- ■ Double outlet left ventricle
- Common arterial trunk
- Congenital anomaly of mediastinal vein
- Congenital anomaly of mediastinal systemic vein
- Congenital anomaly of pulmonary vein
- Anomalous pulmonary venous connection
- ■ Congenital pulmonary venous stenosis or hypoplasia
- ■ Congenital atresia of pulmonary vein
- Congenital anomaly of an atrium or atrial septum
- Congenital anomaly of an atrioventricular valve or atrioventricular septum
- Congenital anomaly of tricuspid valve
- ■ Congenital tricuspid regurgitation
- ■ Congenital tricuspid valvar stenosis
- ■ Tricuspid annular hypoplasia
- ■ Dysplasia of tricuspid valve
- ■ Straddling tricuspid valve
- ■ Overriding tricuspid valve
- ■ Ebstein malformation of tricuspid valve
- ■ Absent tricuspid valve leaflet
- ■ True cleft of tricuspid valve leaflet
- Congenital anomaly of mitral valve
- ■ Congenital mitral regurgitation
- ■ Congenital mitral valvar stenosis
- ■ Mitral annular hypoplasia
- ■ Straddling mitral valve
- ■ Overriding mitral valve
- ■ Dysplasia of mitral valve
- Supravalvar or intravalvar mitral ring
- ■ Congenital mitral valvar prolapse
- ■ True cleft of anterior mitral leaflet
- Congenital anomaly of mitral subvalvar apparatus
- ■ Accessory tissue on mitral valve leaflet
- ■ Congenital unguarded mitral orifice
- ■ Double orifice of mitral valve
- ■ Congenital anomaly of left-sided atrioventricular valve in double inlet ventricle
- ■ Congenital anomaly of right-sided atrioventricular valve in double inlet ventricle
- Common atrioventricular junction
- Common atrioventricular junction with atrioventricular septal defect
- ■ Atrioventricular septal defect with balanced ventricles
- Atrioventricular septal defect with ventricular imbalance
- ■ Atrioventricular septal defect with communication at the atrial level only
- ■ Atrioventricular septal defect with communication at the ventricular level only
- ■ Atrioventricular septal defect with communication at atrial level and restrictive communication at ventricular level
- ■ Atrioventricular septal defect with communication at atrial level and unrestrictive communication at ventricular level
- ■ Atrioventricular septal defect and tetralogy of Fallot
- ■ Common atrium with common atrioventricular junction
- ■ Common atrioventricular valvar regurgitation
- Atypical common atrioventricular valve
- ■ Common atrioventricular junction without an atrioventricular septal defect
- Common atrioventricular junction with atrioventricular septal defect
- ■ Communication between left ventricle and right atrium
- Congenital anomaly of tricuspid valve
- Congenital anomaly of a ventricle or the ventricular septum
- Congenital right ventricular anomaly
- Congenital left ventricular anomaly
- ■ Anomalous ventricular bands
- Congenital anomaly of ventricular septum
- ■ Restrictive interventricular communication when an interventricular shunt is physiologically necessary
- Ventricular septal defect
- ■ Perimembranous central ventricular septal defect
- Inlet ventricular septal defect without a common atrioventricular junction
- ■ Inlet perimembranous ventricular septal defect without atrioventricular septal malalignment without a common atrioventricular junction
- ■ Inlet perimembranous ventricular septal defect with atrioventricular septal malalignment and without a common atrioventricular junction
- ■ Inlet muscular ventricular septal defect
- Trabecular muscular ventricular septal defect
- Outlet ventricular septal defect
- Outlet ventricular septal defect without malalignment
- Outlet ventricular septal defect with anteriorly malaligned outlet septum
- Outlet ventricular septal defect with posteriorly malaligned outlet septum
- ■ Ventricular septal defect haemodynamically insignificant
- ■ Multiple ventricular septal defects
- Functionally univentricular heart
- Congenital anomaly of a ventriculo-arterial valve or adjacent regions
- Congenital anomaly of pulmonary valve
- ■ Congenital subpulmonary stenosis
- ■ Congenital supravalvar pulmonary stenosis
- Congenital pulmonary atresia
- Congenital anomaly of aortic valve
- Congenital subaortic stenosis
- ■ Congenital supravalvar aortic stenosis
- ■ Aneurysm of aortic sinus of Valsalva
- Aortoventricular tunnel
- Congenital anomaly of great arteries including arterial duct
- ■ Congenital aortopulmonary window
- Congenital anomaly of pulmonary arterial tree
- ■ Congenital dilation of pulmonary arterial tree
- Congenital pulmonary trunk anomaly
- Congenital pulmonary arterial branch anomaly
- Congenital pulmonary arterial branch stenosis
- Congenital pulmonary arterial branch hypoplasia
- Absent or atretic right or left pulmonary artery
- ■ Congenital central pulmonary arterial stenosis or hypoplasia proximal to hilar bifurcation
- ■ Congenital peripheral pulmonary arterial stenosis or hypoplasia at or beyond hilar bifurcation
- ■ Congenitally discontinuous, non-confluent right and left pulmonary arteries
- Pulmonary artery origin from ascending aorta
- Pulmonary artery from arterial duct
- Congenital anomaly of aorta or its branches
- Congenital anomaly of ascending aorta
- Congenital anomaly of aortic arch
- Coarctation of aorta
- Congenital anomaly of aortic arch branch
- Congenital anomaly of descending thoracic or abdominal aorta
- Tracheo-oesophageal compressive syndrome
- Vascular Ring
- ■ Anomalous origin of left pulmonary artery from right pulmonary artery
- Congenital arterial duct anomaly
- ■ Systemic-to-pulmonary collateral arteries
- Congenital anomaly of coronary artery
- Anomalous origin of coronary artery from pulmonary arterial tree
- Anomalous aortic origin or course of coronary artery
- ■ Myocardial bridging of coronary artery
- ■ Congenital coronary arterial orifice stenosis
- ■ Congenital coronary arterial orifice atresia
- Congenital coronary arterial fistula
- ■ Congenital coronary arterial aneurysm
- ■ Accessory coronary artery
- ■ Congenital absence of coronary artery
- ■ Coronary arterial hypoplasia
- Congenital pericardial anomaly
- ■ Congenital cardiac tumour
- ■ Pulmonary arteriovenous fistula
- ■ Bifid apex of heart
- Congenital anomaly of position or spatial relationships of thoraco-abdominal organs
You are here: Tetralogy of Fallot with absent pulmonary valve syndrome ⇗ Tetralogy of Fallot ⇗ Congenital right ventricular anomaly ⇗ Congenital anomaly of a ventricle or the ventricular septum ⇗ Structural developmental anomaly of heart or great vessels
| IPCCC Term | Tetralogy of Fallot with absent pulmonary valve syndrome |
| IPCCC Code | 09.05.25 |
| ICD-11 MMS | LA88.20 |
| ICD-11 Code | 1640350515 |
Definition
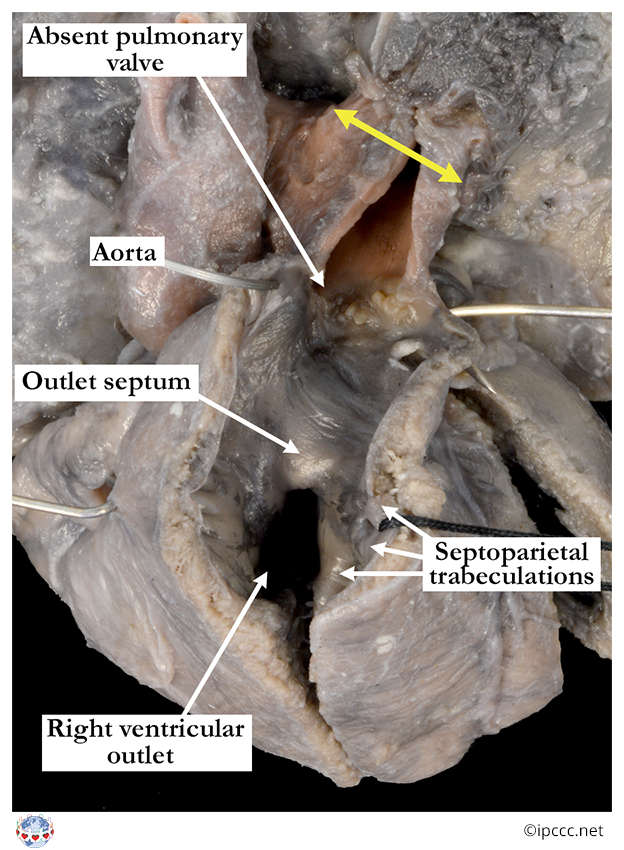
A congenital cardiovascular malformation that is a variant of tetralogy of Fallot in which the ventriculo-arterial junction of the right ventricle with the pulmonary trunk features an atypical valve with absent or rudimentary leaflets (cusps) that do not coapt. In its usual form there is dilatation of the pulmonary trunk and central right and left pulmonary arteries, which when extreme, is associated with abnormal arborization of lobar and segmental pulmonary artery branches and with compression of the trachea and mainstem bronchi, often with tracheobronchomalacia.
 Anatomic Specimen
Anatomic Specimen  Diagrams
Diagrams  Echocardiogram
Echocardiogram  CT-MRI
CT-MRI  Angiography
Angiography  Surgical Images
Surgical Images 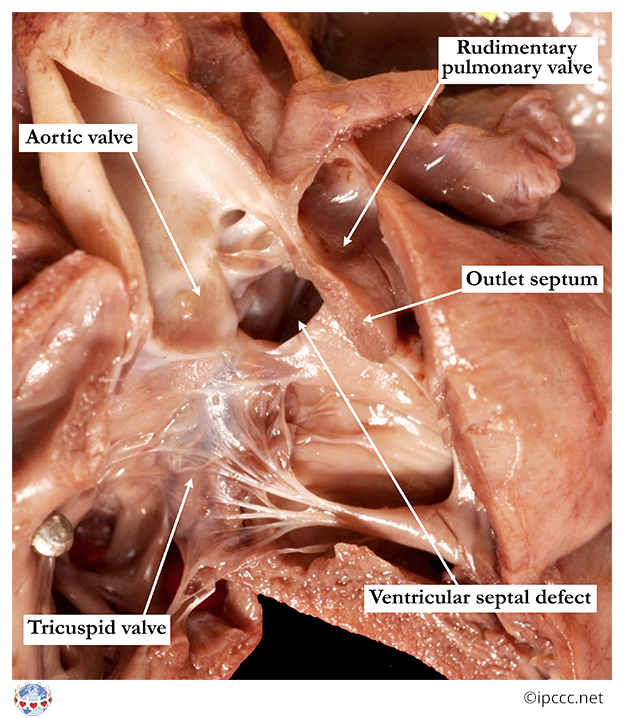
Synonyms/Abbreviations
None
STS-EACTS-derived IPCCC term
Tetralogy of Fallot, Absent pulmonary valve syndrome
EPCC-derived IPCCC term
Tetralogy of Fallot with absent pulmonary valve syndrome
ICD-11 MMS code or crossmap
LA88.20
ICD-10 MMS code or crossmap
**This term is not in ICD-10. If using ICD-10 to code, crossmap to higher order terms “Tetralogy of Fallot”, ICD-10 code Q21.3 and "Other congenital malformations of pulmonary valve", ICD-10 code Q22.3
Parent
Tetralogy of Fallot
Siblings
- Tetralogy of Fallot with pulmonary atresia
- Tetralogy of Fallot with pulmonary atresia and systemic-to-pulmonary collateral artery
Coding Notes
A congenital cardiovascular malformation that is a variant of tetralogy of Fallot in which the ventriculo-arterial junction of the right ventricle with the pulmonary trunk features an atypical valve with absent or rudimentary leaflets (cusps) that do not coapt. In its usual form there is dilatation of the pulmonary trunk and central right and left pulmonary arteries, which when extreme, is associated with abnormal arborization of lobar and segmental pulmonary artery branches and with compression of the trachea and mainstem bronchi, often with tracheobronchomalacia. The physiologic consequence is usually a combination of variable degrees of both stenosis and regurgitation of the pulmonary valve.