|
||||||||
|
|
|||||||||
|
|||||||||
|
IPCCC Code: 01.04.04, 01.03.00, 02.03.01, 02.06.02,
07.02.00, 07.10.00, 01.05.01, 09.29.31 |
|||
|
AEPC Derived Term: |
Double inlet left ventricle (01.04.04) Usual atrial arrangement (atrial situs solitus) (01.03.00) Right hand pattern ventricular topology (D loop) (segmental nomenclature letter 2: 'D') (02.03.01) Aortic orifice anterior right with respect to pulmonary orifice (02.06.02) Right ventricular hypoplasia (07.02.00) Ventricular septal defect (VSD) (07.10.00) Discordant ventriculo-arterial connections (TGA) (01.05.01) Interrupted aortic arch (09.29.31) |
||
|
EACTS-STS Derived Term: |
Single ventricle, DILV, {SDD}, Subaortic RV
outlet chamber with VSD (Bulboventricular foramen) (01.04.04, 01.03.00,
02.03.01, 02.06.02, 07.02.00, 07.10.00, 01.05.01) Interrupted aortic arch (IAA) (09.29.31) |
||
|
ICD 10 Term: |
Double inlet ventricle (Q20.4) Other congenital malformations of cardiac chambers and connections (Q20.8) Ventricular septal defect (Q21.0) Discordant ventriculoarterial connection (Q20.3) Other congenital malformations of aorta (Q25.4) |
||
|
Definition: NA
Commentary: Controversy still attaches to the lesion illustrated in this month's column. There can be no question but that the malformation is well described as showing double inlet left ventricle. It is equally clear from the images that the heart does not have a single ventricle. Tradition has dictated, nonetheless, that the entity was the exemplar of "single ventricle".1 This problem is one of linguistics rather than anatomy, and is circumvented simply by describing the anomaly as being one example of the functionally univentricular heart.2 The only reason that the entity can be justifiably described as having a single ventricle is if the smaller chamber is denied ventricular status. Some still take this stance, having argued that the small chamber is no more than an infundibulum.3 The morphological evidence, however, points to the chamber being an incomplete right ventricle, lacking its inlet component, which self-evidently is committed to the dominant left ventricle.4 If the small chamber were truly an infundibulum, then the entirety of the septum separating it from the dominant ventricle would perforce be the infundibular septum. As can be seen from the images, the septum interposing between the big and small chambers has two discrete components. It is now well established that the apical of these two components carries the ventricular conduction tissues,4 and is nourished by septal perforating arteries.5 It is a true rudimentary ventricular septum. This fact also relates to whether the small chamber should be described as an incomplete as opposed to a rudimentary right ventricle. Both terms are appropriate. The ventricle is incomplete because it lacks its inlet component.6 It is rudimentary because it unequivocally represents the developing right ventricle, as can be seen by the image from the developing mouse heart, in which, like the incomplete right ventricle found in the setting of double inlet left ventricle, the developing right ventricle has yet to acquire its inlet component, but shows obvious apical and outlet parts.
|
|
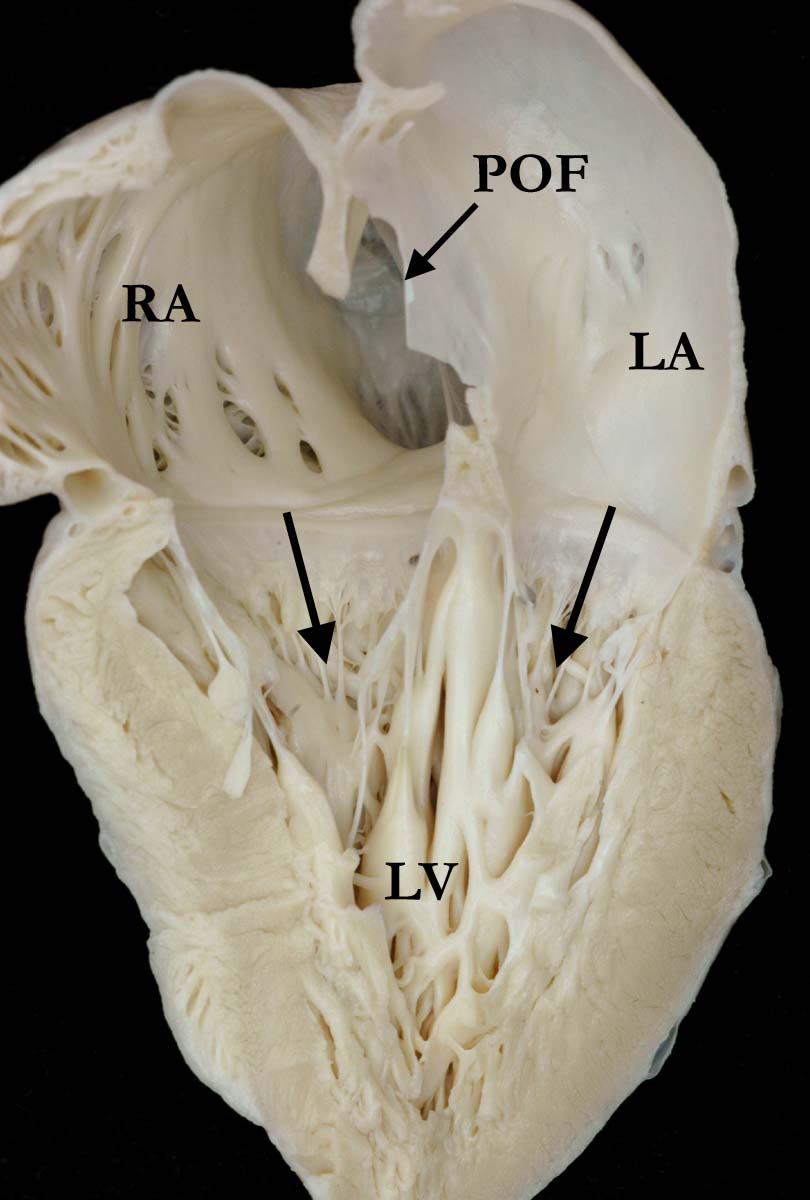
Modality: Anatomic specimen Orientation: Four chamber view
Description: This heart is cut in the four
chamber echocardiographic plane to demonstrate the double inlet
atrioventricular connection (arrows). The atrial chambers are both connected
to the dominant left ventricle (LV),
which is the only ventricular chamber visible. There is an incomplete and
rudimentary right ventricle positioned anterosuperiorly, as shown in the
companion image. The right ventricle is incomplete because it lacks its
inlet component, which is connected to the dominant left ventricle. (POF-patent
oval fossa, RA-right atrium, LA-left atrium) Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A010404-54a Source of Image: Van Mierop Archive, University of Florida, Gainesville, FL Image Certification: pending AWG Rating: pending
|
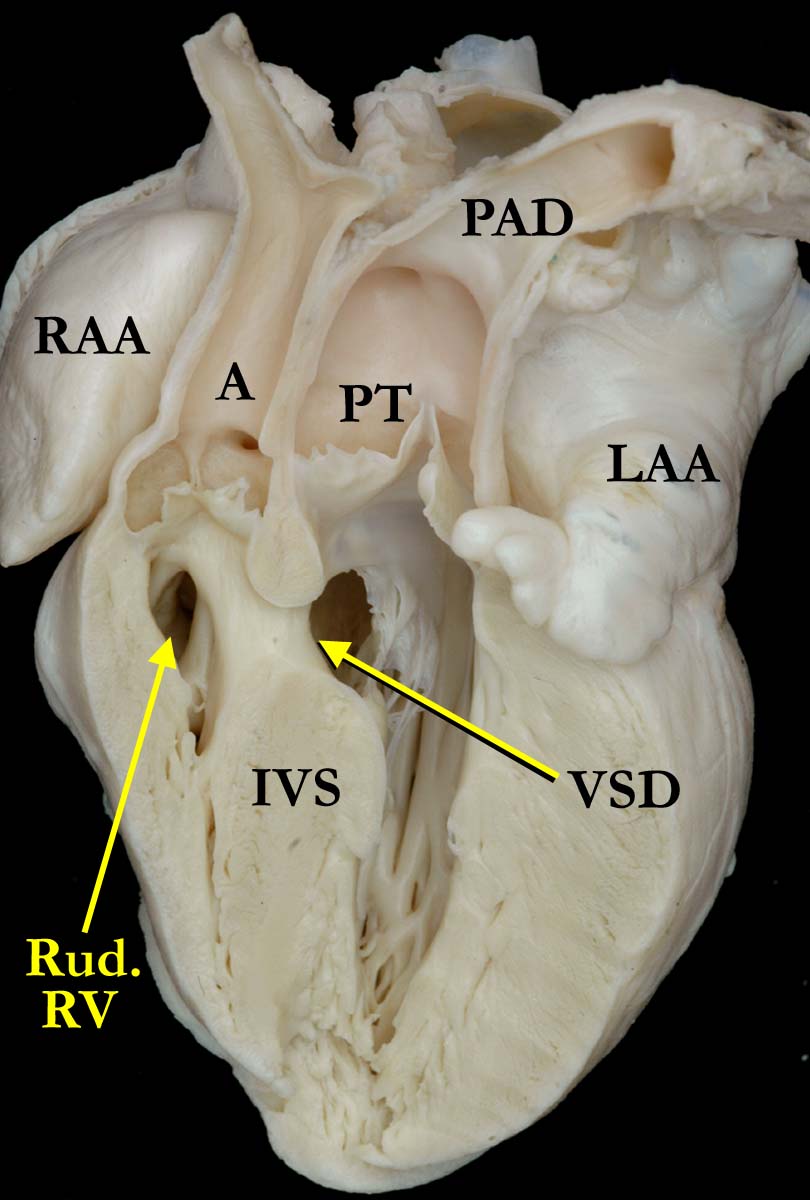
Modality: Anatomic specimen Orientation: Long axis view
Description: The heart, shown in the image
above, has been cut at right angles to the four chamber section. This cut
shows the incomplete and rudimentary right ventricle (RudV) lying superiorly
and in anterosuperior position. It supports the aorta (A), while the
pulmonary trunk (PT) arises from the dominant left ventricle, so that the ventriculoarterial connections are discordant. The aortic arch is
interrupted (not well imaged) and the arterial duct (PDA) is widely patent.
There is a muscular ventricular septal defect (VSD). (IVS-interventricular
septum, RAA-right atrial appendage, LAA-left atrial appendage). Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A010404-54b Source of Image: Van Mierop Archive, University of Florida, Gainesville, FL Image Certification: pending AWG Rating: pending
|
|||
|
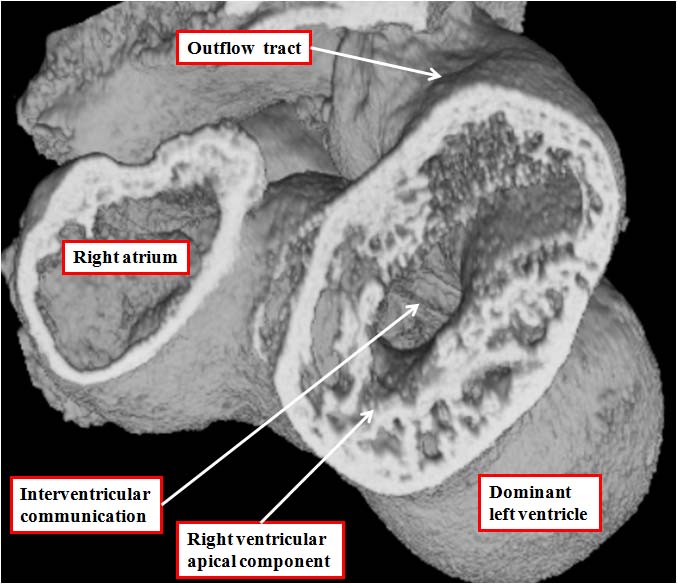
Modality: Anatomic specimen Orientation: Oblique subcostal view
Description: The image shows a developing
mouse heart at embryonic day 11.5. The heart has been prepared using the
technique of high resolution episcopic microscopy, and the dataset sectioned
so as to show the equivalent of the echocardiographic oblique subcostal cut.
As can be seen, the developing right ventricle already possesses its apical
trabecular component, and supports the ventricular outflow tract. At this
stage, however, its inlet is through the embryonic interventricular
communication, the atrioventricular canal being exclusively supported by the
developing left ventricle. The right ventricular chamber at this stage is
analogous to the incomplete and rudimentary anterior chamber found when
there is double inlet left ventricle. The dataset was prepared by Dr. Tim Mohun, Medical Research Council, London, United Kingdom, and the image is
reproduced with his kind permission. Institution: Institute of Genetic Medicine, Newcastle University, Newcastle upon Tyne, United Kingdom Image Label: A010404-54c Source of Image: Timothy J. Mohun, Phd, Medical Research Council, London, United Kingdom Image Certification: pending AWG Rating: pending
|
|
|||
AWG Certification: Pending
|
Copyright ipccc-awg.net All Rights Reserved. Frontpage-Templates.org |