|
||||||||
|
|
|||||||||
|
|||||||||
|
IPCCC: 09.41.03 |
|||
|
AEPC Derived Term: |
Anomalous origin of left coronary artery from pulmonary artery (ALCAPA) (09.41.03) |
||
|
EACTS-STS Derived Term: |
Coronary anomaly, APOC (Anomalous pulmonary origin of coronary), ALCAPA (Anomalous left main coronary artery from PA) (09.41.03) |
||
|
ICD 10 Term: |
Malformation of coronary vessels (Q24.5) | ||
|
Definition: pending
Commentary: Anomalous pulmonary origin of the left coronary artery is a rare congenital defect involving the coronary circulation. It is estimated to occur in 1 of 300,000 live births. If untreated, it results in ischemia, left ventricular dysfunction or infarction accompanied by mitral regurgitation, arrhythmias, and death in infancy in up to 90% of affected patients. The lesion commonly presents in early infancy, and manifests with increasing difficulties in breathing and feeding, accompanied by physical findings of mitral regurgitation and myocardial ischemia. Although there are case reports that date as early as the 19th century, it is Bland, White and Garland, from Massachusetts General Hospital, who are credited as being the first to describe a constellation of clinical observations, validated by the autopsy findings in their patient. The anatomical observation of an abnormal origin of the left coronary artery from the pulmonary circulation provides understanding of the pathophysiology of the disorder. As the pulmonary vascular resistance falls in early infancy, there are incremental changes in symptoms due to the fall in myocardial perfusion. This 'run-off', or 'steal', of blood away from the ventricle, and into the lesser resistance of the pulmonary circulation, decreases myocardial perfusion. It is thought that, if there is insufficient collateralization from the right coronary circulation, myocardial ischemia with mitral valvar dysfunction increases as time passes, and the pulmonary resistance changes. This can ultimately lead to myocardial infarction, with arrhythmias occurring during periods of increased metabolic demand, such as feeding, crying or an intercurrent illness. Although typically the most common origin of the abnormal left coronary artery is from the pulmonary truncal sinuses, the abnormal origin can also be from the pulmonary trunk, or from the right or left pulmonary arteries. In some instances, the left coronary artery can take a normal aortic origin, but then fail to divide, so that either the circumflex or superior interventricular (anterior descending) artery may arise anomalously from the pulmonary circulation. In the most common form, the abnormal coronary artery arises from a pulmonary valvar sinus, as shown in the initial three images, rather than the pulmonary trunk. The traditional acronym for this entity is ALCAPA or Anomalous origin of Left Coronary Artery from Pulmonary Artery (or pulmonary trunk). In most cases, however, this is not an accurate representation of the abnormality. Because of these facts, the acronym favored by the surgeons, namely APOC, or anomalous pulmonary origin of the coronary artery, is the more accurate term. This, however, does not distinguish between anomalous origin of the right, as opposed to the left, coronary arteries. APOLC, or Anomalous Pulmonary Origin of the Left Coronary artery, therefore, would be the better acronym. It is doubtful, nonetheless, whether ALCAPA will ever be discarded. References: 1. J. of Cardiovasc. Trans. Res. (2013) 6:197207. 2. Pediatr Radiol. 2007 Sep;37(9):890-5. 3. Anderson RH, Loukas M. The importance of attitudinally appropriate description of cardiac anatomy. Clin Anat. 2009 Jan;22(1):47-51.
|
|
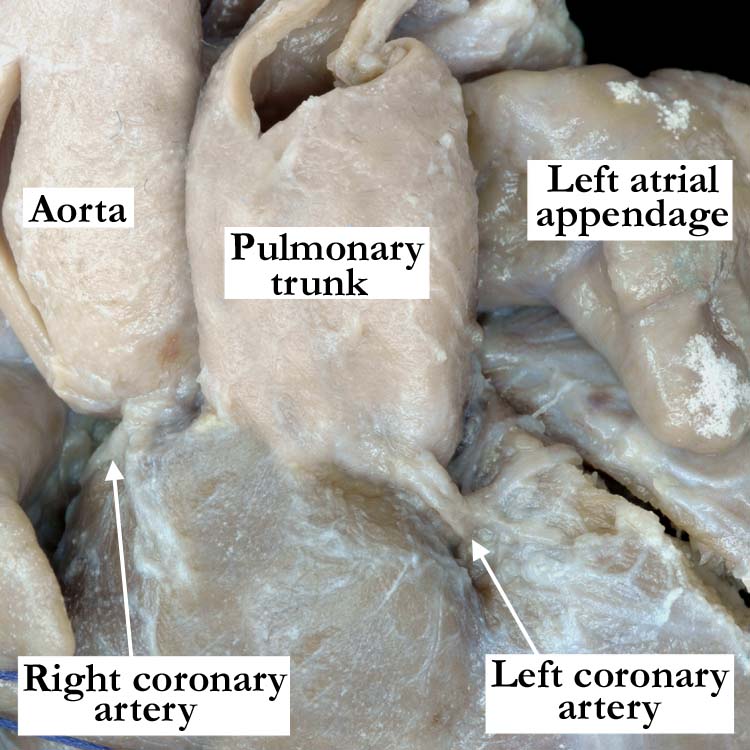
Modality: Anatomic specimen Orientation: Anterior superior view Description: This view of a heart with normally related great arteries demonstrates the normal origin of the right coronary artery from the aorta. The left coronary artery arises from the pulmonary right-handed adjacent truncal valvar sinus. Contributor: Diane E. Spicer, BS Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A094103-152a Image Source: Idriss Archive, Lurie Children's Hospital of Chicago, Chicago, IL Image Certification: pending AWG Rating: pending
|
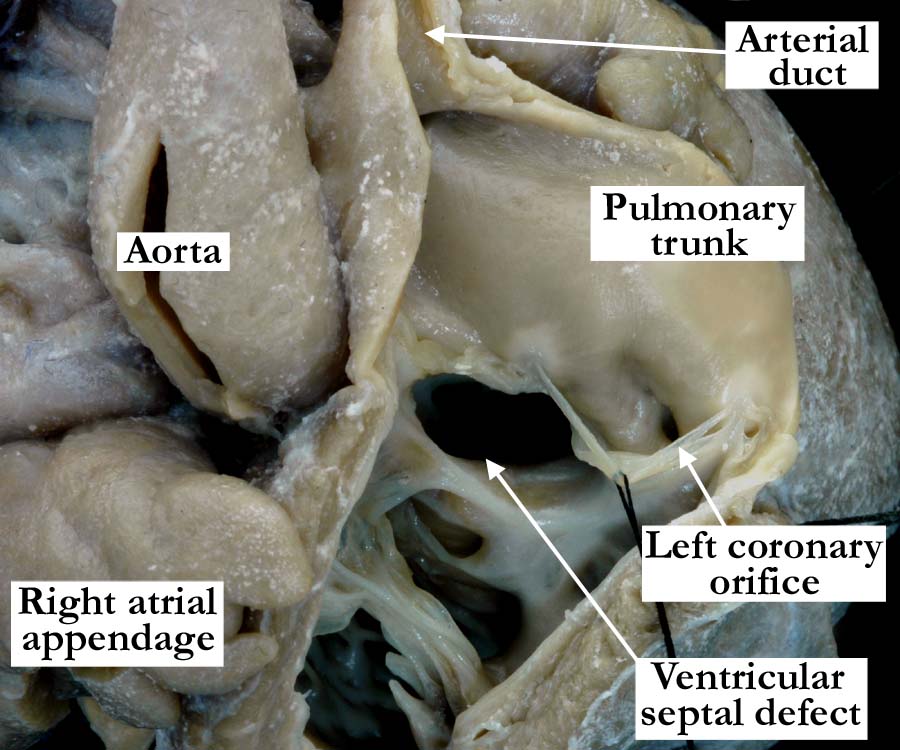
Modality: Anatomic specimen Orientation: Anterior superior view of the right ventricle, outflow tract and pulmonary trunk Description: This view of the opened right ventricle demonstrates that the left coronary artery arises from the right-handed adjacent sinus of the pulmonary trunk. Well illustrated in this image is the presence of a doubly committed and juxta-arterial ventricular septal defect. Although not shown in this image, other findings included signs of left ventricular ischemia, severe aortic stenosis secondary to postero-caudal deviation of the outlet septum, interrupted aortic arch distal to the brachiocephalic trunk. and isolated origin of the left carotid artery from the right pulmonary artery, hypoplastic right ventricle and tricuspid valve dysplasia. Please note the patent arterial duct. Contributor: Diane E. Spicer, BS Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A094103-152b Image Source: Idriss Archive, Lurie Children's Hospital of Chicago, Chicago, IL Image Certification: pending AWG Rating: pending |
|||
|
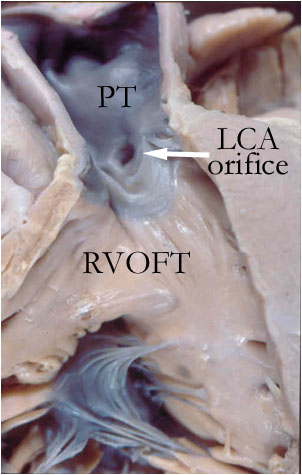
Modality: Anatomic specimen Orientation: Anterior-superior view through opened right ventricular outflow tract and pulmonary trunk Description: In a different specimen, the right ventricular outflow tract (RVOFT) has been exposed to show the anomalous origin of the left coronary artery (arrow) from the right-handed adjacent sinus of the pulmonary trunk (PT). Contributor: Vera Aiello, MD Institution: Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil Image Label: A094103-152c Image Source: Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil Image Certification: pending AWG Rating: pending |
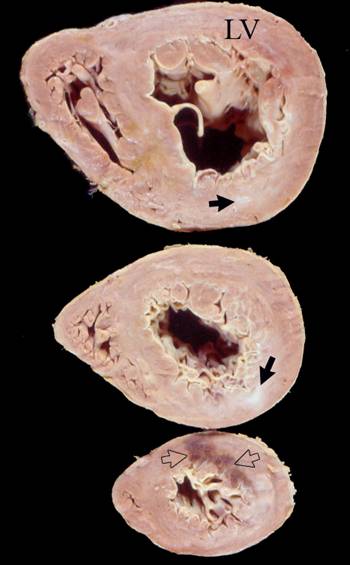
Modality: Anatomic specimen Orientation: Short-axis sections of the ventricular mass Description: In this heart from a child with anomalous origin of the left coronary artery from the pulmonary trunk there are signs of chronic and acute ischemic heart disease. The left ventricle (LV) is hypertrophic and the myocardium shows areas of fibrosis (healed infarction, black arrows) besides an apical area of recent necrosis (open arrows). Contributor: Vera Aiello, MD Institution: Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil Image Label: A094103-152d Image Source: Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil Image Certification: pending AWG Rating: pending |
|||
|
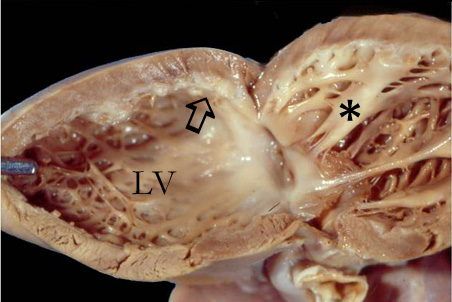
Modality: Anatomic specimen Orientation: Left ventricle opened in clamshell fashion Description: In this heart from a patient with anomalous origin of the left coronary artery from the pulmonary circulation there are signs of long-standing left ventricular (LV) ischemia. There is severe ventricular dilatation and the subendocardial myocardium shows fibrosis (arrow). The supero-posterior (see reference 3) papillary muscle of the mitral valve (asterisk) is pale and fibrotic. Contributor: Vera Aiello, MD Institution: Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil Image Label: A094103-152e Image Source: Heart Institute (InCor), University of São Paulo Medical School, São Paulo, Brazil Image Certification: pending AWG Rating: pending |
Modality: CT Angiogram Orientation: Oblique coronal Description: In another patient with anomalous pulmonary origin of the left coronary artery, the coronary artery arises from the pulmonary trunk, approximately 3 mm above the sinutubular junction, and not from a pulmonary valvar sinus. It runs between the trunk and the aorta to reach the interventricular groove. This is an unusual presentation, as the abnormal coronary artery arises from the pulmonary trunk rather than the more common pulmonary valvar sinusal origin. Contributor: Charles W. Shepard, MD Institution: University of Minnesota Amplatz Childrens Hospital Image Label: CTA094103-152f Image Source: Heart Center, University of Minnesota Amplatz Childrens Hospital Minneapolis, Minnesota Image Certification: pending AWG Rating: pending |
|||
|
Modality: Echocardiogram Orientation: Apical four chamber (uninverted) Description: This echocardiogram is from another patient that as a premature neonate had repair of coarcatation of the aorta. This patient was also known to have a functionally bicuspid aortic valve of no hemodynamic importance. A few weeks after the repair of the coarctation, the patient was noted to have increasing left ventricular dysfunction with increasing mitral regurgitation. The possibility of anomalous pulmonary origin of the left coronary artery was suggested by echocardiography and confirmed at angiography. The presence of decreased left ventricular function and dilation of the left ventricle along with mitral regurgitation is clearly seen on the video hyperlinked to the image above. The angiogram is shown in the next panel. Contributor: Jorge M. Giroud, MD Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: E094103-152g Image Source: The Congenital Heart Institute of Florida (CHIF) Image Certification: pending AWG Rating: pending |
Modality: Aortogram Orientation: Left anterior oblique view Description: An aortogram from the patient described in the previous panel, shows that the right coronary artery (RCA) arises from the right coronary aortic sinus and it is larger than usual. The presumed left coronary aortic sinus, in fact, has no coronary artery arising from it. It can be seen that there is opacification of the left coronary artery (LCA) through myocardial collateral channels. The artery arises anomalously from a pulmonary truncal sinus, with the trunk (PT) filled in retrograde fashion. There is also mild hypoplasia of the transverse aortic arch and a bicuspid aortic valve without stenosis or regurgitation. (Aorta - A) Contributor: Jorge M. Giroud, MD Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: An094103-152h Image Source: The Congenital Heart Institute of Florida (CHIF) Image Certification: pending AWG Rating: pending |
|||
AWG Page Certification: pending
|
Copyright ipccc-awg.net All Rights Reserved. Frontpage-Templates.org |