|
||||||||
|
|
|||||||||
|
|||||||||
|
IPCCC: 07.09.10, 09.15.00, 09.15.28 |
|||
|
AEPC Derived Term: |
Left ventricular outflow tract obstruction: subaortic (07.09.10) Aortic valvar abnormality (09.15.00) Unicuspid aortic valve: unicommissural (09.15.28) |
||
|
EACTS-STS Derived Term: |
Ventricular outflow tract obstruction, Left (LVOTO), LV outflow tract obstruction subaortic (07.09.10) Aortic valve pathology, Aortic valve cusp(s)-modifier for number of cusp(s) = 1 (Unicuspid aortic valve), Unicommissural (09.15.00, 09.15.28) |
||
|
ICD 10 Term: |
Congenital subaortic stenosis (Q24.4) Congenital stenosis of aortic valve (Q23.0) |
||
|
Definition: pending
|
|
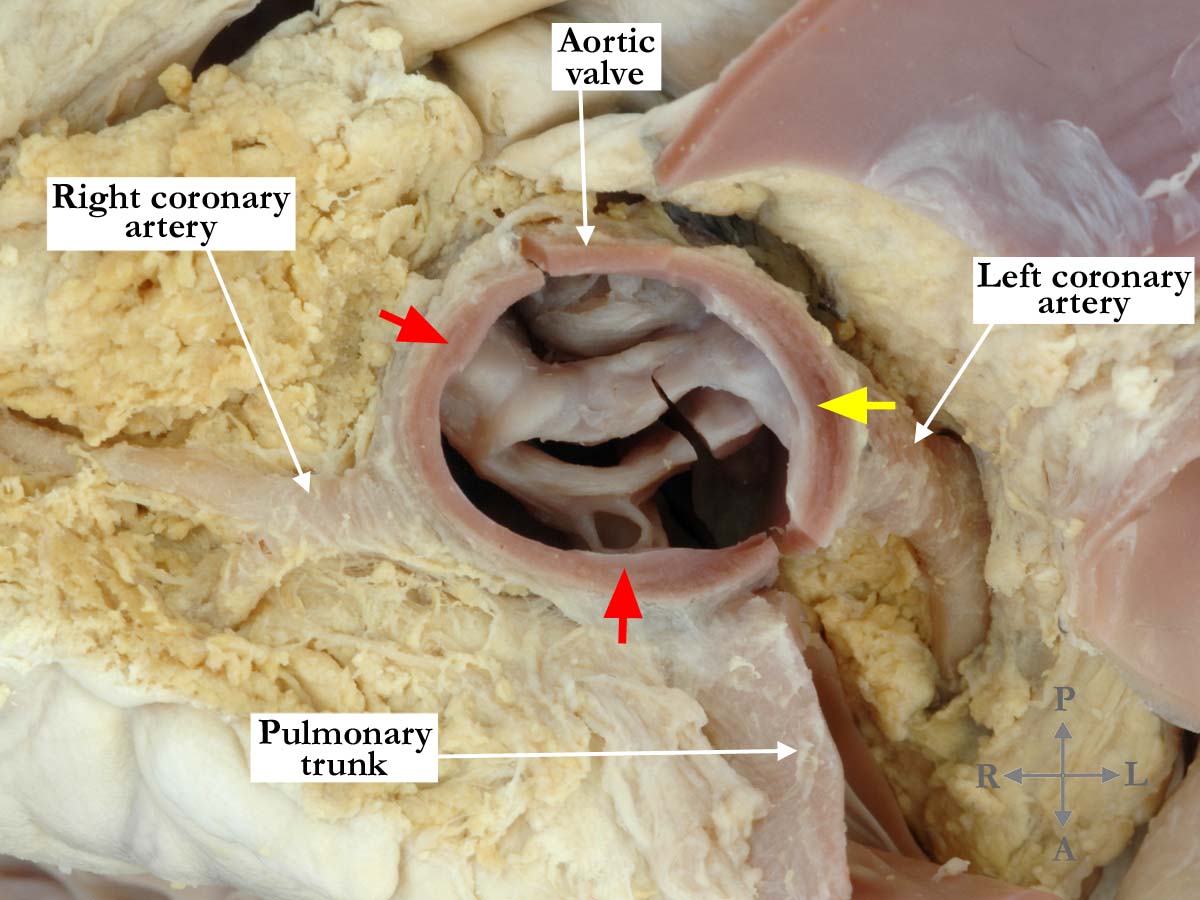
Modality: Anatomic specimen Orientation: Short axis - base Description: This short axis view of the aortic valve shows a markedly thickened, unicommissural valve. The two thickened raphes (red arrows) do not extend to the margin of the valvar orifice while the commissure (yellow arrow) does. There is a solitary opening or zone of apposition within the thickened valve. Within the non-coronary sinus, there is a thickened nodule of firm white tissue that nearly fills the sinus. The left coronary artery exits the aorta adjacent to the commissure (yellow arrow) and the right coronary artery exits near mid-sinus. Contributor: Diane E. Spicer, BS Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A070910-23a Source of Image: Van Mierop Archive, University of Florida, Gainesville, Florida Image Certification: 17 November 2012
AWG Rating:
|
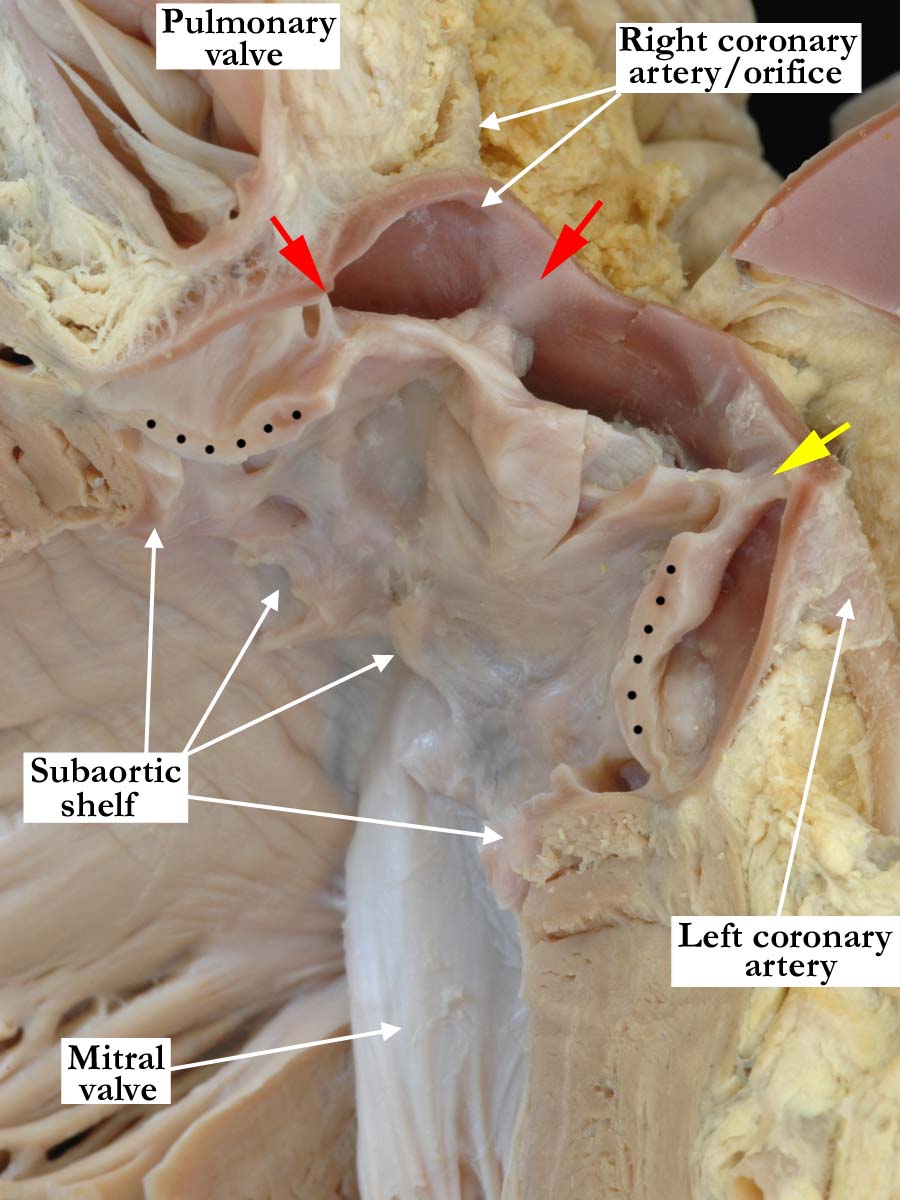
Modality: Anatomic specimen Orientation: Left ventricular outflow tract view Description: The aortic valve is opened and viewed from the left ventricular aspect. There is a subaortic shelf with subaortic stenosis and a unicommissural valve. The cut edges of the valve are marked with black dots. As in the image in panel one, the two thickened raphes (red arrows) do not extend to the margin of the valvar orifice and the commissure (yellow arrow) does. The left coronary orifice exits the aorta adjacent to the commissure. Within the non-coronary sinus there is a thickened, firm, white nodule. Contributor: Diane E. Spicer, BS Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A070910-23b Source of Image: Van Mierop Archive, University of Florida, Gainesville, Florida Image Certification: 17 November 2012
AWG Rating:
|
|||
|
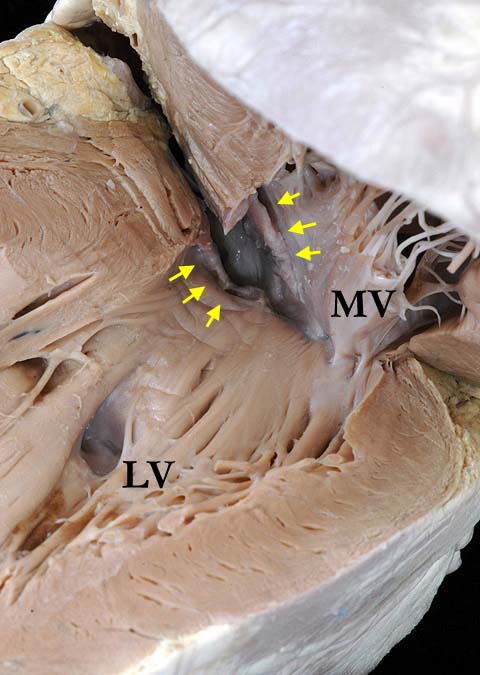
Modality: Anatomic specimen Orientation: Left ventricular apical view Description: A view from the apex, looking into the left ventricular outflow, shows the fibrous ring (yellow arrows) that causes the severe subaortic stenosis. (LV - left ventricle, MV - mitral valve) Contributor: Diane E. Spicer, BS Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A070910-23c Source of Image: Van Mierop Archive, University of Florida, Gainesville, Florida Image Certification: 17 November 2012
AWG Rating:
|
These pathological images of an abnormal aortic valve generated a lenghty discussion about how to distinguish unicuspid/unicommissural aortic valves from bicuspid ones. With permission from the participants, we publish the following excerpts:
This aortic valve looks more to
me like the unicommisural and unicuspid variant. The solitary opening within
the valve does not extend to the margin of the valvar orifice and most
commonly, extend(s) backwards to the zone of fibrous continuity with the
mitral valve. This is the typical appearance of the so-called unicuspid and
unicommissural variant. In most cases, the solitary zone of apposition
point(s) towards the mitral valve. In this example, it is running from
right to left. This is unusual in my experience, as is the fact that the
zone of apposition does not extend to the sinutubular junction
we can only
describe what we see!. The subaortic shelf is very nicely shown.
This is often called a membrane, but as Dr. Jane Somerville has emphasised
on numerous occasions
the obstructive lesion is far from membranous. As
shown in this specimen, it is a discrete fibrous shelf. It can often be more
extensive, and then forms the so-called tunnel variant. I agree
that this looks like a
unicommissural valve. This is commonly mistaken for a bicuspid valve by
echocardiographers and angiographers because of the length and shape of the
orifice. This differs from typical, isolated pulmonary stenosis which
usually has a circular orifice in the center of a domed valve; whereas
unicommissural AS typically has an eccentric elliptical orifice.
Regarding terminology of fibrous subAS (and PS in TGA) there are some
others as well. I like the term "discrete" when there is a linear
"membrane-like" obstruction. In my experience "tunnel" is usually what
happens
after surgical resection. There is also fibrous subAS from
abnormal attachment of an AV valve to the septum or crest of a VSD as in
common AV canal. Similar to the current cases, these are often acquired
after (AV) canal repair. There are also ball-like excrescences from mitral
valve chords and accessory mitral valve leaflets that can cause fibrous
subAS. I also think it looks unicommissural and that is often mistaken by echocardiographers. Essentially most critical AS infants have unicommissural valves. |
|||
AWG Page Certification: 17 November 2012
|
Copyright ipccc-awg.net All Rights Reserved. Frontpage-Templates.org |