|
||||||||
|
|
|||||||||
|
|||||||||
|
IPCCC: 09.29.33, 09.30.01, 09.29.31, 09.30.02, 07.10.01, 07.17.06 |
|||
|
AEPC Derived Term: |
Interrupted aortic
arch between subclavian & common carotid arteries (type B)(09.29.33) |
||
|
EACTS-STS Derived Term: |
Interrupted aortic
arch (IAA), Type B2 (Interruption between the carotid and subclavian
arteries with both subclavian arteries arising from the aorta distal to the
interruption) (09.29.33, 09.30.01) |
||
|
ICD 10 Term: |
Other congenital malformations of aorta (Q25.4) Other specified congenital malformations of peripheral vascular system (Q27.8) Ventricular septal defect (Q21.0) Congenital malformation of cardiac septum, unspecified (Q21.9) |
||
|
Definition: pending
Comments: Interruption of the aortic arch is known to occur at three specific sites, namely at the isthmus, which is between the left subclavian artery and the descending aorta, between the left common carotid and the left subclavian arteries, or between the right and left common carotid arteries. The first two variants are much commoner than the third option, with the variants also known as Types A through C, using the classification produced by Celoria and Patton. The lesion is also known, however, to co-exist with anomalies of the subclavian arteries, and these additional malformations can make the situation more difficult correctly to interpret. In the images shown, it might seem that the interruption is between the right and left common carotid arteries, with the ascending aorta supplying the right brachiocephalic artery. In reality, the interruption is between the left common carotid and left subclavian arteries, and there is additional retroesophageal origin of the right subclavian artery. Even more rarely, it is possible to find this type of interruption with isolation of the right subclavian artery, in other words with the subclavian artery arising from a pulmonary artery via a patent arterial duct, so the diagnostician needs to be aware of all these potential pitfalls. In addition, the branching pattern typical for the right aortic arch can be seen with either a left brachiocephalic artery, a retroesophageal left subclavian artery, or an isolated left subclavian artery. All known cases with the branching pattern typical for the right-sided aortic arch have DiGeorge syndrome. The case is also of interest because of the morphology of the associated ventricular septal defect. Interruption itself is often associated with lesions that reduce the flow through the ascending aorta. When found with a ventricular septal defect, then the defect is usually of the malalignment type, described by some as a conoventricular defect. Such defects, as in this case, can be perimembranous. Their main feature is the posterior deviation of the muscular outlet, or infundibular, septum, which then obstructs the subaortic outlet from the left ventricle. On occasion, the septum can be fibrous rather than muscular, and the defect then becomes doubly committed and juxtaarterial. Perimembranous defects, of course, are not always associated with malalignment of the muscular outlet septum, nor are conoventricular, or malalignment, defects always perimembranous. In this particular case, the defect becomes perimembranous because there is fibrous continuity between the leaflets of the mitral and tricuspid valve, so the atrioventricular conduction axis will be at potential risk in the postero-inferior margin of the defect. (Reference: Celoria GC, Patton RB. Congenital absence of the aortic arch. Am Heart J. 1959 Sep;58:407-13)
|
|
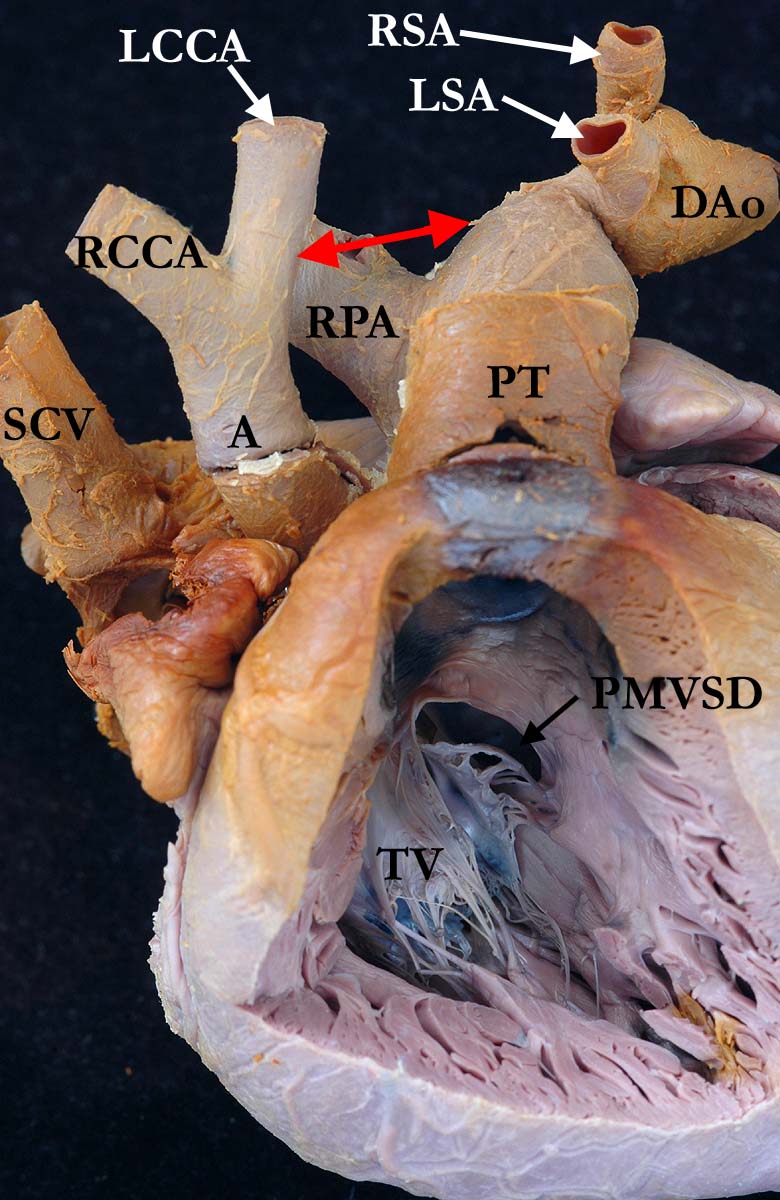
Modality: Anatomic specimen Orientation: Right ventricular view Description: This view shows the anterior, anatomic view of the right ventricle and great vessels, the free wall of the right ventricle has been dissected away. The tricuspid valve (TV) can be seen in the inlet. A perimembranous ventricular septal defect (PMVSD) extends into the outlet portion of the right ventricle, an alternative term is a malalignment ventricular septal defect. There are concordant ventriculo-arterial connections, the aorta (A) and pulmonary trunk (PT) normally related, with a hypoplastic ascending aorta. The aorta is interrupted (red arrow) between the left common carotid (LCCA) and the left subclavian (LSA) arteries. There is distal retroesophageal origin of the right subclavian artery (RSA). (DAo-descending aorta, RCCA-right common carotid artery, RPA-right pulmonary artery, SCV-superior caval vein). Contributor: Diane Spicer, BS Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A092934-20a Source of Image: Van Mierop Archive, University of Florida, Gainesville, FL Image Certification: 4 Feb 2012 (rediscussed 3 March & 8 September 2012)
AWG Rating:
|
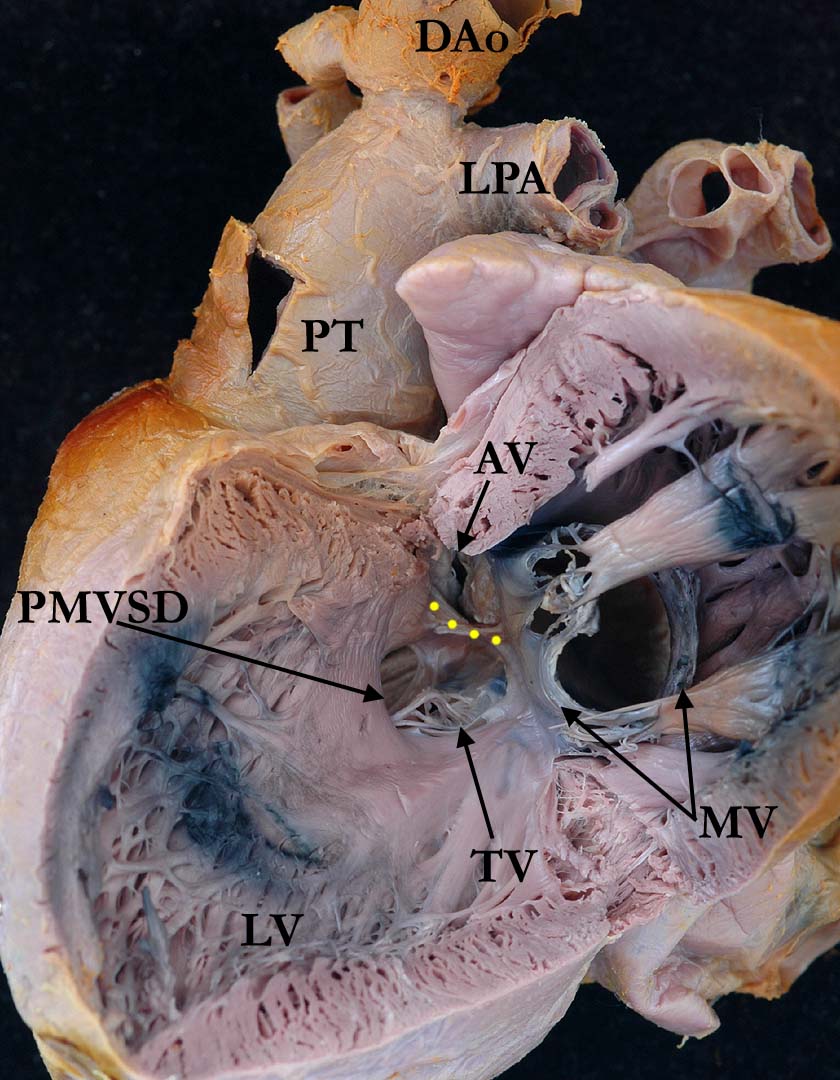
Modality: Anatomic specimen Orientation: Opened left ventricle in clamshell fashion Description: This view shows the septal surface of the left ventricle (LV), revealing the posterior malalignment of the muscular outlet or infundibular septum (yellow dotted line), which indicates that the perimembranous defect (PMVSD) is of the posterior malalignment type. The malalignment also encroaches markedly on the subaortic outflow tract, and almost certainly produces obstruction. The tricuspid valve (TV) can be seen through the ventricular septal defect and is in fibrous continuity with the mitral valve (MV). (AV-aortic valve, DAo-descending aorta, LPA-left pulmonary artery, PT-pulmonary trunk). Contributor: Diane Spicer, BS Institution: The Congenital Heart Institute of Florida (CHIF) Image Label: A092934-20b Source of Image: Van Mierop Archive, University of Florida, Gainesville, FL Image Certification: 4 Feb 2012 (rediscussed 3 March & 8 September 2012)
AWG Rating:
|
|||
AWG Page Certification: 4 Feb 2012 (rediscussed 3 March & 8 September 2012)
|
Copyright ipccc-awg.net All Rights Reserved. Frontpage-Templates.org |